Patients imagine someone is watching out for them
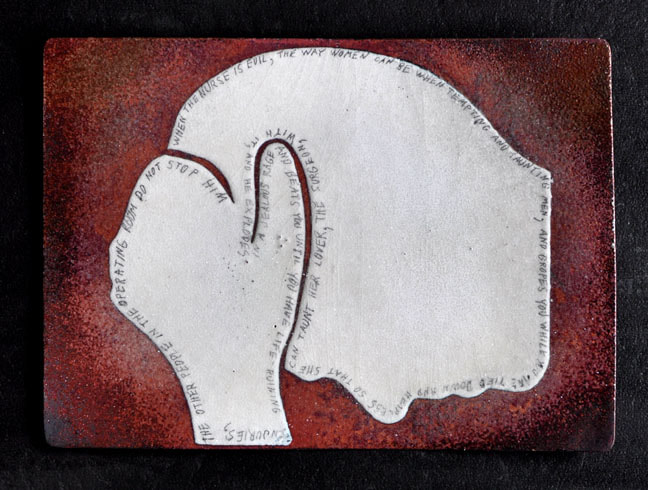
I prefer making art that is more subtle than this, but you can be pushed to where you just blurt something out. Like this piece. The words penciled along its border can be read if you click on it and scrutinize its larger version. But to save you from straining your neck and eyes to read that, here is what it says:
“When the nurse is evil, the way women can be when tempting and taunting men, and gropes you while you are tied down and helpless so that she can taunt her lover, the surgeon, with it, and he explodes in a jealous rage and beats you until you have life-ruining injuries, the other people in the operating room do not stop him.”
Maybe I’ll make a larger one so that there is room to add that they also don’t call security. They also don’t make a record of it. They also don’t ask you if you are all right. And they also only are doing what is normal when things go wrong in medicine. They learn not to any of those things. The institution doesn’t want there to be a memory or record of anything negative. The hospital wouldn’t even let me file a complaint. They don’t want any information to exist that could hurt their rating. Not even if it would protect future patients, or perhaps give the current one some hope of getting the injuries treated.
It was true 250 hundred years ago. It is true now. It probably still will be true 2000 years from now if people keep trying to solve such problems within the ancient paradigm in which everyone always has tried to solve problems in medicine (about which I’ve written elsewhere). So I made this out of material that will last that long. There are artifacts thousands of years old made this way. Today they call it vitreous enamel, but no one understands what that means. It means that it is glass melted onto metal. It is a technique that humans learned even before the discovery of blacksmithing.
Usually this is done in a kiln or furnace. I do it with a torch, which takes practice. I melted the white glass onto copper. When it cooled I etched the glass to have a tooth like paper so I could pencil the words along the border of the white area. Then I melted a layer of clear glass over that. Graphite doesn’t fade. And now it is encased in glass. If no one smashes it, it will be here to speak for other victims of crimes in medicine 2000 years from now. Perhaps I should have put a date on it to help to correct the assumption victims usually jump to about these things – that medicine didn’t used to be this way. It always has been this way (see Dr. Benjamin Rush on another site).
I created this one only because a nonprofit had requested small works of art they could auction to raise money. I was working on them when one the the shills sent by the nurse’s lawyer arrived trying to befriend me in order to get me to say something they could use to drag me back into court. Anything oral they would alter to their purposes. But I finally blurted out a response in this piece and then wrote this page in response to further questioning from her.
* * *
I would prefer saying no more about it. It’s fine with me if you stop reading right here, but so many doctors and police officers and medical board investigators and lawyers and such have required me to explain why a surgeon would assault a patient, and I am so tired of explaining it as they stare at me as though it is tiresome to have to listen to the answer, and I am so tired of being interrupted and told to wrap it up when the answer takes more than three sentences. It would not have to take more than three if information like this got out often enough for people to have some basic knowledge about crime in medicine, but the medical community is amazingly successful at preventing that. So I am putting this page on this website where, from now on, the link to it can be one of the three sentences they allow me, but I’ll need only two. “Go to this link. I cannot bear to repeat it one more time.”
They only are looking for an excuse to disbelieve it anyway. I have had them dismiss me saying that a doctor would have no reason to harm a patient. In this day and age, bullshit as shallow and ignorant as that is believed in medicine? Yes. As though lust and jealousy and anger and other sociopathologies do not exist in medicine. As though no nurse ever before groped a patient and no doctor ever intentionally disabled one. As though there never has been a book or paper about about serial killers in medicine. As though no doctor ever groped or raped a patient. As though the statement, routinely repeated in medicine, that a doctor would have no reason to hurt a patient, were unassailable. It goes a long way to making clear chasm between what health care providers choose to believe and the world they make their patients live in. So, of the many motives doctors have for injuring patients, I guess I have to explain the specific one this doctor had for intentionally ruining the life of this one.
———————-
In this case, it was a nurse who pushed the doctor over the edge. Unwittingly I had primed him. Not on purpose. Trying not to is something I’ve had to deal with my whole life. But there are guys like the good doctor everywhere.
I first tuned into it in grade school. I was an obedient, peaceful child with no interest in being the alpha male. So why so often did I get singled out by boys wanting to fight? At first, adults I asked about it suggested that it might be because I always was the tallest person in the class. Perhaps that made me the target for boys wanting to prove themselves. But over the years I finally noticed a pattern. These things happened after I had made people laugh.
For a long time I wasn’t aware that I made people laugh more than others did, but others were aware of it. With a group of boys on the playground during recess, I’d be one of the more silent ones as the bullies and braggarts ran things. Then I’d mutter an aside that would send the group rolling in laughter. Eventually, I figured out that the one who did not laugh would be the one who would pick a fight with me later. Unfortunately, it is something boys don’t grow out of.
Like when I got to be an adult and was standing in the isle at the Cincinnati Playhouse in the Park during intermission when a woman I knew stopped to say Hi. During the three minutes that we spoke she laughed more than she talked. When she turned to walk back to her seat her date did not follow immediately. Instead, he stepped into my space glaring, with nostrils literally flaring, gritting his teeth, clenching his fists, all the clichés, as he was a cliché by this point in my life, making sure that I understood that he was the alpha male. I’d been through this enough times to know that it was because I had made his girlfriend laugh. Maybe he never had been able to do that. I don’t know.
Like when I was at my sister’s for dinner and her brother-in-law had brought a new date. Late in the meal I said something funny. Apparently I had said a lot of things that were funny that evening, because someone said that I really should find someplace where I could be funny for a living. The new date of the brother-in-law agreed saying, “Yeah. Like maybe in my apartment.” The mood in the room changed abruptly.
My sister’s brother-in-law and I had been semi-friends until then, but after that moment he would spend the rest of our lives treating me as though I could not possibly be of enough consequence to warrant his even acknowledging my presence. Like decades later at his father’s funeral when I complimented him by saying that he gave a nice eulogy. He looked down, turned his back to me, and walked away without saying a word. Frankly, it was a self-inflating eulogy. I only had been trying to be polite. But making someone’s girlfriend or wife laugh can have permanent consequences.
Enough people had said to me that I should find a way to get paid for being funny that one time I let someone drag me to where I could look into that. There was a comedian an hour away with a regular gig in a comedy club. He needed material. Every week he gathered would-be comedians to sit in a circle on the floor to brainstorm material. To entice people to come he offered lessons and opportunities to get on stage. A guy who owed me a favor thought that this would be the favor he owed me – taking me there.
We sat on the floor in a circle following the comedian’s lead. One of the things he had us do was to take turns coming up with a word or phrase that would be funny at a specific point in his routine. The person to your right would offer a suggestion. Then you would. Then the person to your left would.
We were trying to think of a name or a description for a character in a new story the comedian was trying out. After a few rounds a guy across from me said, “Ricearoni.” The next several people said entirely unrelated things, but when it got to me, I said, “The San Francisco Treat.” The comedian laughed and wrote that down. It was going in his act.
The guy across from me looked at me accusatively and said, “I already said that.”
“You did?”
“Yeah. I said Ricearoni.”
“Oh. O.K.”
“I did. That was mine.”
“O.K.”
“It was. I said it first.”
“I’m not arguing with you. It’s yours. Sorry.”
Saying “Ricearoni” is entirely different than saying “The San Francisco Treat” in that context. I got the idea to say it because of what he said. That is the purpose of taking turns throwing out thoughts – to feed off each other. But he wanted the credit for it. It’s not as though we were getting paid or getting our names in a program. If he wanted it, he could have it.
Still he still wasn’t happy. He wanted to take this outside. He appeared as though he might have been a football player two or three years ago in high school. He was shorter, but probably outweighed me by 50 pounds – a sturdy, powerful guy who was ready to fight because I made a comedian laugh. Guys like these are everywhere. Even in operating rooms.
As I got older, I tried to get better at avoiding being funny. But I never think that what I am about to say is funny. It is hard to edit it out when you don’t see it coming. I needed to because when you make people laugh, people nearby start paying attention and the circle paying attention to you widens. In a minute or two you can be the center of attention in a room in which there are other people who thought they deserved to be the center of attention. Sometimes they hate you for that.
Like when you are lying on an operating table with an open incision in your abdomen and an IV in your arm, but only under a local anesthetic so that you are conscious. When you are making quips in response to the operating room staff’s conversation and everyone is laughing except the surgeon, perhaps it is time to pause being funny. The surgeon had started interrupting me. It was clear he was one of those guys who has to be the alpha male. He resented not being the center of attention even for a moment.
I resolved not to say anything else funny, but there was something in the IV that was relaxing me. I needed to be wary and cautious, but some drug was relaxing me and undermining that. One of the nurses was going to go to a casino for the first time in her life. She had never tried gambling before. The nurses began talking about that. I muttered something about gambling, the nurses laughed, and this time the surgeon said something stern about how to gamble, but he didn’t have the nurses’ undivided attention. He stopped the operation, demanded everyone listen to him by saying, “I’m serious now.” And he explained the correct way to gamble. I knew, I suspected everyone knew, what he was saying was nonsense. There is no correct path to follow to beat the casino. When he finished, unfortunately I made one more quip. I said, “This is great. Get operated on and get gambling tips all at once.” In context it was the funniest thing I had said so far. The operating room staff let loose with the loudest collective laugh yet. And that was when the nurse decided to make the surgeon jealous by letting him see that she had been groping me throughout the course of the procedure, actually from even before the procedure had begun, as easily can be done from her position during an inguinal hernia repair. Up until then it was clear to me that groping patients was something she did all the time. She was so well practiced at it. And had started even before the surgeon had entered the OR.
As the laughter was dying down, the nurse who was groping me rocked back on her heels to laugh one more time in a way that caused her to lift her hands enough for what she was doing to me to be exposed. I was mortified and wondered who she would have wanted to see this. She made the surgeon jealous by letting him see that she had been groping me throughout the course of the procedure, actually from even before the procedure had begun, as easily can be done from her position during an inguinal hernia repair. Up until then it was clear to me that groping patients was something she did all the time. She was so well practiced at it. It had started even before the surgeon had entered the OR.
It was not during the biggest part of the laugh. It was after the peak, when the laughter of the group was subsiding, after she had regained her composure. You know how you can hear when a baby is faking a cry to get attention? The nurse’s laugh was like that. She faked one more and rocked back on her heels as though it was her laugh that caused her to rock back lifting her hands so that what she was doing to me would not remain hidden. I was mortified and wondered who she could want to have know about this. Then I found out.
Both she and the surgeon were married to other people, but apparently there was something going on between them because that’s when the surgeon exploded. It was the surgeon’s buttons she was pushing now. I already had suspected she was a button pusher because of how she had pushed mine. Pushing his moved it beyond suspicion.
He had been standing at my left hip, but stepped around to where he was between my legs. Probably bracing himself with some tool, like an army navy retractor, he bent down like a line backer driving all his weight into a practice sled on a football field, but driving the tool into my taint so hard it knocked me off of the table. I didn’t know until that moment that they tie you down when they operate, to make sure you don’t fall on the floor. So, I didn’t.
I was swinging by the strap around my hips, my head swinging near the floor. I was worried about getting a head injury, at least after the first blow. He dragged me back onto the table and did it again. It was so violent I then worried about whiplash. He did this perhaps a dozen times. When he finally stopped, the OR was silent. All chatter had stopped. The few faces I saw were drawn and dark.
And so I learned that when a surgeon explodes in a jealous rage and beats you until you have life-ruining injuries, the other people in the operating room do not stop him. They don’t call security. And they don’t report it. I also learned that afterwards no one else in medicine will treat the injuries lest the diagnoses be used in a complaint or a grievance that could hurt a colleague. They don’t tell you they won’t treat them. They just don’t find them.
They were life-ruining. They consumed so much of my time and money, especially when the nurse sued me to shut me up, that I lost my health, my wife, my retirement, and my ability ever to get another girlfriend (so you probably can guess what physical ability was targeted and destroyed). And a doctor would never have any reason to harm a patient, right? It took years to get the diagnoses, but my lawyer did not show those to the jury and did not let me tell the story above in court. He had a conflict of interest and got me sued (for one thing he refused a pre-trial settlement I told him to accept, but it gets much worse than that).
If you are reading this to find out what the injuries are and how I got them, you could stop here.
Below is just more details about the injuries and what it took to get them diagnosed.
Over and over physicians I went to for treatment for the injuries asked me how I knew I was assaulted. How did I know? Seriously? I explained it in every way that I could. Eventually, I learned (someone let me find out) that the surgeon and my primary care physician were calling them ahead of time and telling them not to diagnose the injuries.
I went through the phases injured patients go through. I just wanted help for the first years during which I deteriorated further. When it became clear that it was more than just the myths universally believed in medicine that made it impossible to get treated, I began just trying to get any mention of it into the record. But the records I got from the hospital were too illegible to discover who had been in the operating room. I could get no records at all from my primary care physician. He made up lame excuses for why he could not give them to me, initially telling me that HIPPA laws would not allow it and later refusing to obey a subpoena delivered by the Sherriff, and after that refusing to obey a subpoena from the Ohio State Medical Board. As with many injured patients, in the beginning I just wanted to do what I could to prevent other injured patients from going through all this. The mendacity surrounding me prevented me from getting care, prevented me from gaining knowledge, prevented me from getting records or anything but the rattling sabers of defamation suits from the hospital, which had started the first time I tried to get help. It finally pushed me to the last place injured patients end up. I wanted a lawyer’s help.
I have written elsewhere about the fact that only one in some thousands of injured patients can get a lawyer, and that the ones who do almost never get anywhere with it. I called every single lawyer in the phone book. One med mal lawyer (as medical malpractice lawyers are known) explained to me why no one ever would help me or almost any other injured patient, information for which I was extremely grateful. But then there was this one other lawyer.
John Metz had what might have been the most prestigious office in the city of Cincinnati. It was the penthouse of the Carew Tower. He had fought med mal cases all the way to the State Supreme Court and won, eventually doing that 14 times.
When I called him he asked how many doctors I had been to. I had been asked that enough times to know that simply answering that question with a number would be the end of the conversation. So I said, “How can any injured patient get a doctor to diagnose the injuries?”
He said, “I tell people to go out of town.”
“I can do that?”
“Yes.”
“Where?”
“I tell people to go to the Mayo Clinic.”
“But my doctor calls ahead to tell people not to help me.”
“Oh. No. Don’t tell your doctor you are going.”
“I can get in without a referral?”
“The last thing you want is a referral. Here is what you have to do. You have to research exactly what kind of a doctor you need to see for your specific injuries. Then you make an appointment with that doctor. But you have to go as a cash customer. You cannot use your insurance or take any records (this was before electronic records) because all the people you have seen so far have a connection to the people keeping you from getting diagnosed. And you cannot use insurance because that can make it possible for them to trace back to what is happening to you now. You want to arrive there saying that you brought no records with you because you just want a fresh opinion. You want a second opinion unfettered by any previous opinion. And you have to make sure you do not complain about anything. Do not look anything but grateful for all the wonderful care you know you are going to receive there. Smile. Be charming. Be friendly. No matter what they ask you, you have to be a happy camper who just wants a second opinion. If you are not friendly and charming and grateful, you only will get more of what you already got.”
That advice eventually became the foundation of what I told to thousands of injured patients over the years as they kept calling me, the only guy they ever had heard of who figured out how to get his iatrogenic injuries diagnosed.
I did not go straight to the May Clinic. I knew I needed to rehearse this. I needed to discover the pitfalls. I needed to find the ways all this could go wrong. I did that first at New York Presbyterian Hospital where I had an appointment to see a Dr. Eid. Within five minutes of entering his office I was receiving one of the first tests I would have received the first time I asked for help if anyone had wanted to help me – Doppler ultrasound with dye.
He had asked me what had happened to me. I describe the violent assault and what the problems had been ever since. He ushered me into another room and told me to do my best to get an erection. He stuck his head in the door a minute later to toss magazines to me of naked people. Do people really need these things to get turned on? These were so graphic that, to me, they were off-putting.
When he returned and began the test he showed me, live, on the screen what some of the injuries were and what they meant for me going forward. I had never heard the term “venous leak.” In short, a penis is full of tiny balloons that fill with blood and cause it to swell. When they are full they can be popped with impact. When they are not full they cannot. But once popped, they are forever popped. So they leak. If enough of them leak, they no longer produce enough swelling for a viable erection.
He pitched me on a surgery he could do that would be like implanting a synthetic replacement for an erection. He said the surgery is ninety-five percent successful, but it would mean living with something like an erection 24 hours a day from then on. I later asked another surgeon about it and was told it was, at best, thirty percent successful. Insurance won’t even cover it.
When I got home I called the surgeon’s office and asked the nurse who answered to mail to me a copy of the records of my visit with Dr. Eid. When they arrived he had lied and written in the record that I said that the problem came on gradually over a period of time. Even from another city he protects my assailant. I wrote back a letter complaining about that.
The second place I went out-of-town was The Boston University Medical Center where there was a Dr. Goldstein who had written a book about the parts of the body that on me were injured. I spent months trying to get an appointment. It finally became clear to me that I was being given the run-around. The surgeon I was asking to see did not want to see me.
I got discouraged and gave up for two or three months. Everywhere I turned doors were slammed in my face one way or the other. I finally tried Boston again. The nurse recognized my name but enough time had passed for her not to remember why. She apologized for having lost track and scheduled an appointment. So by luck and forgetfulness I got the appointment that she previously had worked to prevent.
911 occurred shortly after getting the appointment. The two planes that destroyed the World Trade Center (the World Trade Center was where I routinely caught the shuttle to the airport when I used to fly in and out of NYC on a regular basis) had flown out of Logan Airport in Boston. Two weeks after 911 friends looked at me like I was crazy to be flying into Logan airport at that moment. My thinking was that at that moment it might have been the safest airport in the country with how alert everyone there would be now. Still it was a little spooky in the airport there.
I spent a night in a hotel. In the morning I went to Dr. Goldstein’s office. They told me to have a seat in the waiting room. He would be with me soon. I waited for hours. Finally a man stepped into the room, asked me if I was Joel Selmeier, then motioned for me to follow him. Was this Dr. Goldstein?
In his office he peppered me with questions. Some were about why I had come to Boston to get diagnosed. I told him that I had been unable to get diagnosed in Cincinnati. I told him why and that I needed to escape the influence of my primary care physician.
The person I was talking to turned out not to be Dr. Goldstein. It was a psychiatrist who was checking to see if I was crazy. In his notes he wrote that my story did contain some paranoid elements, which would be the information about people working behind the scenes in Cincinnati to make sure I did not get diagnosed.
When I finally was taken to Dr. Goldstein’s office he was being shadowed by a group of students. He asked if I minded if they observed. I did not care.
He asked me question after question, including why I had come to Boston to get diagnosed. I told him I just wanted a fresh opinion unfettered by any previous opinion. He said that could not be why I was here and kept up the interrogation.
Finally, he asked how I knew I was assaulted. Nowhere else have I ever met people who ask questions with that confounding construct. It is a form of question common in medicine. It assumes you are too stupid to accurately observe your own experience. I have never had that same kind of question asked of me by anyone other than health care professionals.
Like, one time, when I became single again, I met a nurse at an event. We have agreed to meet at another event in a week. It wasn’t really a date. We just had a nice conversation and wanted to have another. I called mid-week to confirm we both still were going to it but spent the five minutes on the phone with her angrily interrupting every sentence I began to say. I didn’t know her well enough to be treated like this. At the next event she asked why I was so quiet. I said I was waiting to see if she still were going to be interrupting me. She said she never interrupted me. I reminded her of our phone call. She asked, “How do you know I interrupted you? I never interrupt anybody. I didn’t interrupt you.”
“How do you know I interrupted you?” The assumptions inherent in the mind of the speaker about both parties to that question say so much about the mindset of health care professionals – all of it bad.
Now, yet another surgeon was asking how I knew I had been assaulted. All I could think was that no oral articulation of the answer to that ever had succeeded in getting me past this point. I had tried every articulation I could think of. I had practiced them. I had written them down and rewritten them. Now, because of this question alone, all of the years, the money and the work to get to this appointment would be for nothing once again. The months spent getting this appointment, the flight here two weeks after 9/11, spending the night, waiting half the day, all for nothing again because of this same question that, as far as I can figure out, cannot be successfully articulated. Frustrated, I snapped.
Charm went out the window. I leapt from my seat and threw myself into his desk like a linebacker driving into a practice sled on a football field. I did it again and again, each time the things on his desk jumping, rattling, and sliding, each time my thinking they would fall on the floor and break. After the sixth or seventh time I stood up and loudly said, “How do you know I assaulted your desk?”
While attempting to duplicate the assault by assaulting Dr. Goldstein’s desk, he did not change expression. He sat quietly watching me batter his desk. He is quite charming really. He also is the first doctor who did not write lies in the record to discredit me and protect my assailant, which is what is normal in medicine and is what happened with every other doctor I had been to. Apparently, answering that unanswerable question required abandoning words and demonstrating the assault. “How do you know I assaulted your desk?” What articulation could answer that. I had tried, “I was there. It happened to me. I was awake and talking and being groped. Are you going to ask how I knew I was being groped?” Nothing I ever said worked for anyone in medicine. The question only is a demonstration of how deeply they believe their own self-serving myths and disbelieve anything a patient could say that might undermine them.
Where it Counts
Dr. Goldstein not only didn’t make up lies, but he further diagnosed the injuries, even putting his finger on the point at which, according to the x-rays, the blows must have been struck so that I would understand where the injuries were – between my legs, on my taint, explaining why I could hardly sit down for so many years, and never was able to get an erection again, apparently the goal of the good doctor. The assault even caused a collar injury to my urethra making it difficult to urinate for the rest of my life. There were multiple problematic injuries beyond that. I did not even know that an erection extends that far inside the body. Wouldn’t you think my lawyers would have brought up any of that at trial to protect me? It was in evidence. But the jury never heard anything to indicate that I have any injuries at all. My lawyers were Catholics. Successfully defending my suit would have uncovered yet another Catholic institution covering up sex abuse, so they didn’t.
I lost a decade to being a fulltime seeker of treatment at first and then to being a fulltime defender of the lawsuits brought to shut me up. The nurse whose groping started the whole thing got rich by suing me. The glee with which she leapt from her seat in court upon hearing that she now was going to become rich, by taking everything I had, was one of those moments you’d like to clear from your mind. She turned to look right into my eyes in triumphant glee. That’s a person with no empathy and no remorse. That’s the definition of a psychopath. According to people who study that field, psychopaths have an 80% recidivism rate. And she’s still out there – safe in her career and now rich.
You, as a patient, need to be worried about the people like that who are in medicine, but no one can warn you about them. I cannot warn you about her. One of her best friends is a lawyer with a reputation for being unprofessional and unscrupulous. The least vulgar thing I ever heard any other lawyer say about him is, “He’s a piece of work, isn’t he?” He told my lawyers to tell me that he took this personally and vowed to maintain a vendetta against me for the rest of my life. And he has. That is violation of his professional ethics for which the state bar could punish him if I were not too beat up to pursue it. (PTSD is a strange thing to experience. The necessary documents can be sitting in front of me. I can look at the words on the pages, but I cannot read them. It was the lawsuit filed by the good nurse that gave me a small stroke and then the PTSD that haunts me for the rest of my life.)
So the nurse pushed his buttons too. And pushed her husband’s buttons. It appears that her husband is the one who signed up my email address at hundreds of penis enlargement sites to flood me with vile spam. Unless that too was her lawyer. It had been a valuable email address. It was joel@joel.com. Repeatedly, I had been offered a lot of money for that email address, enough to buy a small house. There were several people who called every year hoping I’d change my mind. Now it was worthless because of the amount of spam in which people on her side buried it.
In spite of all of the injuries they caused to my body and my marriage and my finances, I hadn’t thought about making artwork about any of them. I have enough trouble inventing reasons to keep breathing. If breathing didn’t happen naturally, I would let it stop. At the time of this writing, twenty times a day I am in one kind of pain or another because of what they have done, but I was trying not to be. I was trying to forget. But her lawyer keeps invading my life over and over. He keeps persuading unsuspecting people to befriend me and try to get me to say something they can use to drag me back into court. He persuades them that I’m some kind of demon who must be stopped from ruining the life of this poor, innocent nurse.
Creating artwork is what I do as naturally as I breathe. So the vitreous enamel above came as naturally as a yawn one time when one of their shills was trying to get me to say things about what happened in the hospital (I didn’t – I never do). I was making rough drafts of vitreous enamel pieces to donate to a non-profit organization that auctions them to raise money to put inner city kids to work during the summer. One of the lawyer’s shills was pestering me, trying to get me to use words that would give the nurse legal grounds against me, but instead I wrote words on that vitreous enamel piece that don’t. He and she finally got me to say something, just not what they wanted.
Several times a year they sent someone to try (usually young blonde women who are charming and pretend to be sympathetic). The next time it happened I wasn’t making vitreous enamel. I was making making models for a sculpture when their intrusion focused me on the nurse again. I was trying to move on, but they wouldn’t let me. The shill asked, “Can you tell me what happened to you in the hospital?” No. Not on the phone. I need a written account of what is said so that the nurse’s lawyer will have a more difficult time distorting it and making up lies to use to drag me into court. If you really must know my story, this page is the only account I’ll give. And now there is sculpture helping to express it.
[A picture of it was here but disappeared when moving to a new server]
This is a paper model of what would be 11 feet tall and made of steel. If I make it there might be a couple of smaller versions of it in front of it, like children or grandchildren, to make this bird-like piece appear to be so innocent and wholesome that it would not occur to anyone looking at this predator that the bug it is about to eat is you. Like the nurse for whom I’ve named the piece “RNFA” for Registered Nurse, First Assistant.
On hand I didn’t have pieces of steel large enough to make it, nor the time to make it. But there is no hurry. It’s not as though they are going to leave me alone. I’ve made many of pieces of art in the years since they first disabled me, and since they prevented me from getting treatment before the injuries had become inoperable scar tissue – which eventually I learned is the routine in medicine after they injure you. And many pieces since they sued me for complaining about it – all without a single piece of art being about them, until finally the vitreous enamel above. And now this model for a sculpture.
I guess their continuing to invade my life year after year finally broke some barrier. So now there is more art about them – this model of a sculpture named for the nurse. And a third and a fourth model have been made, all pieces designed to be around 10 feet tall, one about the surgeon, and one about the hospital. Thematically unified works can end up being a show. Wouldn’t you think they’d want to stop stoking the fire and just go away?
Instead they have caused me to have thoughts about pieces about other characters involved in the story. I don’t have to think up excuses to make art, only to go on breathing so that I’ll be here to do it.
That is how successful medicine is at shutting down the patients it injures. They beat the patients up so badly that the patients don’t even want to live, so that they will give up and go away. Thousands of injured patients called me over the years asking for help with getting their iatrogenic injuries diagnosed. Rumor had spread that I was the one person who had figured out how. My wife hated this. Sometimes she would step into my home office and glare at me. Seven days a week they called. Twenty calls in a week would have been a slow week. It could be Saturday afternoon and my wife might have been hoping we could do something together, but I had stepped away from lunch for forty-five minutes to try to help some desperate patient.
Sometimes they called from anonymous phone booths and refused to divulge even what state they were in for fear of getting sued. The rattling sabers of risk management are very effective (and invisible to treatment providers who turn out to be unaware of this). Between the threats and punishments, injured patients become unable to warn you about a nurse who is a career sex predator and a surgeon who, if you say the wrong thing on his operating table, will ruin your life. Since no one gets to learn the lessons that victims learn, only victims know important parts of what must be known about medicine to make it safe for patients. But injured patients do not have anyone they can tell.
Now that there are electronic records, I cannot help other injured patients get treatment. There is nothing they can do now to escape what is put in their records. False records are created to stymie them and protect the injurers at the expense of the injured.
Traveling to another country might work for injured patients, but who can arrange that? And I have made myself less accessible while continuing to work on it. Telemedicine with India has some promise now that it is the case that all a patient needs in order to get images or blood work authorized is the National Provider ID Number of the physician ordering it. That might work as long as the people receiving such orders do not check the patient’s record first, which happened to me more than once when trying to get images made on the order of a local doctor before I was experienced enough to know how to dupe the receivers of the orders into being less suspicious of the reasons for them. It still would take a savvy and adroit patient to pull it off. Injured, suffering patients, trying to raise their families and manage their careers as well as managing their new health problems are not in a position to devote their entire lives and finances to working that out like I had to in order to learn what I learned.
Medicine is resolutely in denial of all of this. I have never met a person in medicine who, when questioned, was not. I also have never met one who would entertain the suggestion that he or she might be in denial.
Patients never understand what is going on. Injured ones rarely can explain what happened to them. The ones who try get worn down trying to explain it to health care professionals who appear either not to hear them or not to believe them. By the time injured patients called me, they were prepared for more of the same and didn’t know how to do anything but tell their life story ending with the event that was the subject of the call. This almost never was as short as fifteen minutes. Calls lasting twenty or thirty were normal. Sometimes they were much longer.
The first thing I always asked injured patients to do was to get their records. They almost always were shocked to find there was no record of the original injuries, and none made subsequently by the people to whom they went for treatment.
Once a patient is injured in medicine, whether accidentally or intentionally, the first priority of the entire medical community is to make sure there is no record of it and make sure no one ever finds out, no matter what they have to do to patients to arrange that.
When the police finally went to the hospital to look into it, they told me they wanted to dismiss the case because there was nothing in the record about it. Did the police imagine that the person who committed the crime was going to enter in the record that he had?
It took some arguing to get them to relent. So they went back again and this time the surgeon told the police that he had a witness who would testify that nothing happened. His witness was the nurse who started the whole thing. The police already knew she had caused the assault. I had written that into the charges that I filed. They had refused to let me file charges against her, so in the charges against the surgeon I explained what she did to cause him to explode like that. “Wrap it up,” they said as I was writing it. They didn’t want more than three sentences either.
So I didn’t get to say it in much detail, but it’s there. The police didn’t want to do this job. So they let her, the person who caused this, testify saying that the surgeon didn’t assault me. So in my community the police let Bonnie testify for Clyde and on that basis closed the case.
That apparently helped bolster the confidence of the nurse and her lawyer. This was yet another agency shutting me down. So the nurse then sued me for defamation. In court her attorney persuaded the jury that I didn’t say she had any part in the assault until after the police told me she would testify for him, but of course it was right there in writing in the charges I had filed before the police went to the hospital, which was before we even knew her name. All my attorney would have had to do to correct that lie is point that out, as I asked him to do. “Asked” is putting it mildly. I argued, actually shouted, during recess right in the courtroom, as he shouted back to prevent me from finishing sentences. And if he wasn’t going to do that, then would he please point out that the truth about what she did also was stated in the account of the crime on my website that was put there long before I got the police to let me file charges. That account was the basis for this suit in the first place and was in evidence. But my attorney would not point out that either. You really shouldn’t hire an attorney who is a member of the same religion as the hospital, or rely on a primary care physician who is also. Especially when that religion already is roiling from scandals involving the covering up of sex abuse in communities the world over.
I wasn’t a child when members of that religion abused me. I was an adult taking notes. Can you imagine how much they wanted to silence me about a case that shows how pervasively its community contributes to the cover-ups? My attorneys did not bring my expert witnesses (I’d offered to pay for them myself), did not subpoena documents I had demanded they subpoena, did not depose witnesses I demanded that they depose, and did not correct lies told in court by the nurse and her lawyer that easily could have been corrected.
Like when the surgeon, my assailant, testified for her in court saying that neither he nor my primary care physician could find any physical reason for my complaints. In fact, the diagnoses of those injuries were in evidence as part of the site they were suing me for creating. All that needed to be done to prove that the surgeon was lying was to point out that he had been given copies of those diagnoses.
In addition to those out-of-state diagnoses, I also had in-state, hostile witnesses who would testify that my primary care physician had called their office and told them not to treat me, witnesses my religious attorneys “failed” to depose or bring to court in spite of my imploring them to do so.
Or like when her attorney said that on my web site I said that in full view of the other personnel in the operating room she took my penis out and masturbated it. That word did not appear on my site. I said nothing of the kind.
He demonstrated it for the jury by running his hand up and down an imaginary phallus several feet long and bigger around than my arm saying that this is what my web site said she did right in front of everyone else. It did not say that. And my attorneys refused to correct that. We argued about it, but they refused.
I asked my attorney to point out to the jury that they could read the web site and see for themselves what it said. If the jury read the copy of my site that was in evidence, they would see for themselves who was lying – something an attorney actually trying to defend me would have thought to do himself. It had been printed out and entered in evidence. I argued with my counsel trying to get them to do that. I also argued and demanded that they make sure that the jury looked at the actual site. But my attorney didn’t. And the jury didn’t. The only version of it they ever learned was the fowl, salacious lies invented by her attorney.
My attorneys did not even raise an objection when the surgeon who assaulted me said on the witness stand that neither he nor my primary care physician could find a physical reason for my complaints. That was him testifying for my primary care physician who was not present for us to cross examine. You cannot do that. Objecting to that is a no-brainer. But I could not get my attorneys to object to it.
I also could not get them to point out that the person who was giving this testimony was the person who committed a violent crime and did anyone really expect him to testify honestly?
Her lawyer impugned every thing about me that he could, suggesting that I wasn’t even any good as an artist. I had a copy of an article from the Cincinnati Enquirer that I tried to get my lawyers to present. This is its beginning.
The Cincinnati Enquirer
Monday, March 31, 2003
Bats Incredible! … Some of Cincinnati’s top names are participating, including Zaha Hadid, Joel Selmeier, Holly Schapker, Ted Gantz, Marcia Burke, Cole Carothers, Michael Sharp, Matt Kotlarczyk, Mark Fox, Scott Jones, Jimmy Jones. . . .
enquirer.com/editions/2003/03/31/tem_monlede31.html
Zaha Hadid is an internationally renowned architect and artist who designed the new Contemporary Art Center in Cincinnati. My architect brother had been telling me about her for years, he was so impressed with her work. I’m listed second after her in this list of top artists in Cincinnati. But my attorneys wouldn’t present it or mention it. I only was able to get one of them to say that I wouldn’t be getting all of this if I weren’t any good. All of what? What did the jury learn? My lawyers wouldn’t mount an adequate defense even of that?
How can I define this as anything other than being sabotaged? I kept passing notes to them during the trial, as I was supposed to, telling them things to do to defend me, things to which they were supposed to respond, but they never did. (After the trial when I got my case file, none of those notes were in it – isn’t that a failure to keep work product?) Even when I was on the stand I had to object myself when my attorneys would not. Yet I kept trusting them. Just like I trusted my nurses and doctors.
There had been a pretrial settlement offer for an amount for which I could have written a check. It was not a small sum, but it was a sum for which I was prepared. I had the check in my pocket. I had money ready for this. I had told my attorneys to accept the settlement, but they rejected it. When I was not present they rejected it. They literally got me dragged into court against my wishes by “failing” to accept the settlement offer that I had ordered them to accept.
They even delivered to her a private document that her attorney used to beat me up in court. That document was enlarged and put on an easel in front of the jury and left there day after day. I wanted to create a document to replace it. I had sign-making materials and tools at home. I could create a display that night and bring it in the next day. I wanted to make a copy of a page from the website that shows what and where the injuries are. But my attorneys refused to let me do it. So the private document sat in front of the jury day after day with the word “Accusations” at the top of the list of pages on which there were statements that I thought should be checked by my attorneys. My attorneys never checked them. Now the private document was being used to vilify me and my counsel wouldn’t even let me replace it with something in that would help my case, like artwork that would show the jury that the injuries were real.
I did not understand what was going on at the end of the trial when the judge asked if there were any orders. It turns out that is when my attorney can argue that the monetary award should be thrown out, or the verdict thrown out, or the case appealed or even thrown out. The only person who can do that is my personal attorney. My insurance company’s attorney cannot do it, so instead he stood next to my attorney saying loudly enough for the judge and jury and me to hear that the monetary award should be reduced if not thrown out. He repeated that the nurse had no monetary damage, no days of work missed, no therapy expenses, no missed promotions. And yet the jury decided to be made whole she deserved 1.3 million dollars from me. He said that is an enraged jury acting out of passion and should be thrown out. My attorney stood silently and did not say a word.
So, my insurance company’s attorney reminded him that the trial had been brought to a stop for half a day by juror misbehavior. The one juror who wanted to know what my site actually had said had looked it up online and went back to the jury saying what the site does and does not say, and especially revealing that it says that nurses never report these things and so are no reliable witnesses. She was neutered after that. The only juror trying to find the truth was silenced. That ordeal makes this verdict appealable. But my attorney did not repeat what all of us heard and so the judge could not rule on that.
My insurance company’s attorney also pointed out that he had delivered a private document to the plaintiff’s attorney that was blown up and left on an easel for days in front of the jury. That was appealable. But my attorney did not say a single word. The just sat waiting patiently for quite a while before finally dropping his gavel to end the case.
Then my attorney persuaded the appeals attorney assigned to the case after we lost, to let the insurance company’s attorney handle the appeals issues (or so I gathered from the appeals attorney who later said he wished he had handled it himself). My insurance company’s attorney had never read the website (he didn’t even know how to log onto the internet or use email) nor learned the facts of the case. How could he handle the appeals issues? It would be a black eye for the insurance company’s attorney to let it be revealed how badly he had handled it. Did someone expect him to give himself a black eye? He didn’t appeal it.
Long prior to her filing the suit I had tried and tried to get my attorneys to submit to that nurse a copy of everything I was intending to put on the internet so that she could okay with it before it was posted. She was not the only one I to whom I tried to get my lawyers to submit such documents. I didn’t know who might sue me, but I did not want to get sued by anyone. My attorneys never did it. If they had this suit could not have been filed.
Finally after a long time of their not submitting this document to the people I listed, in exasperation I sent a four page fax (since emailing him was impossible) to both of my attorneys explaining why it needed to be done and imploring them to do it, but they still didn’t do it. So she sued me saying it was because she was worried about what I might post on the internet. That is what the suit was about – what I might post in the future. She wouldn’t have been able to file that if my attorneys had done what I repeatedly implored them to do. There are multiple counts here on which these two attorneys should be held accountable.
A legal malpractice attorney wanted to do that. It looked like a slam dunk to him. He wanted to sue my attorneys for doing this to me, until he learned that because I had been a full time patient and defender of lawsuits I had not had any income for a few years. The only thing for which a lawyer can be sued is loss of income and in three years I hadn’t had any to lose. So he told me to file a grievance. I wanted to, but PTSD has made me incapable. Try as I might, I cannot read the documents. That is reliving it again. My mind will not do it. I’m doubly disabled now – physically and spiritually. I would need some volunteer to help me go through the records because I cannot do it one more time.
These two attorneys were my last hope. It was so hard to learn that I could not trust them, harder than it was to learn I could not trust my health care professionals. It took so long. Isn’t one of the main purposes of art enabling others to learn what you learned without their having to go through it themselves? Now I am better at recognizing when someone isn’t really helping. All people should be better at that. If more patients were, perhaps fewer of them would get injured or bankrupted or killed in medicine. Of course, preventing most of that only would require honest information being available to patients. But when things go wrong, there isn’t any of that in medicine.
The state medical board investigator could not learn even who was in the operating room. The people in the OR were the witnesses. The hospital would not tell him who they were. He didn’t try to find out beyond asking if they would tell him. And they wouldn’t. If they had, it only would have made waves at the state medical board where he worked. He asked who the witnesses were only because I demanded that he find out. I had tried myself and they wouldn’t tell me. They told him they didn’t know and he left. But of course they knew.
Hospitals are required to tell you who your caregivers were, and they do, unless they don’t want to. There is no one in charge of making them obey such regulations and no penalty for violating them. When I asked the police to do something they said, “What do you want us to do about it?” I had been naive enough to think that when people break the law, the police will to do something about it.
When I finally managed to force the police to let me file criminal charges against the surgeon, even though they would not let me file them against the, as yet unnamed, nurse, they finally went to the hospital and did one thing (and possibly only one) that would have been done by any medical board investigator who both knew how to do the job and cared enough to do it. The signature of the nurse who groped me was on the post op report, but it was illegible. The police showed it to other nurses until one of them both recognized it and didn’t lie. At last we had her name. And then the surgeon told the police that that nurse, the one who caused this whole thing, the one who had groped me and whose name we just had discovered, would testify that this never happened. And that was good enough for the police.
The patient community needs an agency that is on its side and knows things like how to determine the names of caregivers and that the police are unmotivated and that state medical boards are obstructive, and all the other things that injured patients learn one at a time by being defeated by them. It needs an agency that already has thought about how to protect patients in the face of that. I keep coming across other patients who have had to learn the lessons the way I learned them. I’ve seen worse cases than mine. And there are public examples, like serial killers in medicine. Our health care industry does not even protect us from serial killers, honestly. For instance, Charles Cullen (opens a new tab linked to another site where there is a list of similar examples). From the top down in his hospital people covered up for him while he murdered patients. That is the routine. Even for lesser sins. They even cover-up permanent incompetence.
Meanwhile patient safety advocates worry about errors. Errors. Only errors. Anything worse turns out not to be discussable. It would be too disrespectful to caregivers. Health care professionals brush worse things off saying, “That’s another matter entirely.” Really? In a discussion about patient safety, intentionally injuring patients is another matter entirely? And refusing to treat injuries even if only accidentally incurred is another matter entirely? And treatment providers so talentless at their jobs that they routinely injure patients are another matter entirely?
Patient safety advocates say that we have to keep on good terms with health care. They imagine treatment providers can be persuaded or educated or managed into being more compassionate and more attentive so that they will fix the problems they create for patients. (Sometime I will write about having watched my primary care physician, right in front of me, rearrange his beliefs to secure his own emotional comfort at the expense of my physical well-being. There are things that can not truly be understood without having watched that.) This is an effort that has been going on since Hippocrates 2,300 years ago. All indications are that it will keep going on for the next 2,300 without anyone ever stopping to think that maybe it is time to think differently about how we think about medicine and our treatment providers.
There is a National Task Force on Violence Against Health care Providers, but no such entity trying to protect patients. There is no one on the side of injured patients. No agency representing us. No one we can call who is not advocating for the people who injured us (of the patients with legitimate grievances only one in some thousands can get a lawyer making that an unrealistic option). So we must smile and pretend to be happy campers in order to get medical people who don’t know where we’ve been to give us routine care in a world where health care professionals can prey on patients in all the ways that they do, not only with impunity, but within a culture that enables them to persuade themselves that they don’t do that.
Some people want to pass laws requiring treatment providers to report accurately. Where is lucidity? Lost in the silence of those who cannot speak, those who will not report, those who do not investigate, and those who cannot think outside the box of what is comfortable for those in medicine.
I have less than half the money I would have had for old age if they had not ruined me. I also don’t have the wife I would have been able to share old age with because of this. My four worst injuries were caused by treatment, not just this crime. And the things I have to do to nurse the injuries take up a major portion of each day. Meanwhile, without my permission, my body keeps breathing.
But there is no point in responding to “How are you?” with anything other than “Couldn’t be better. You?” In my new reality sometimes I respond by saying, “Perfect.” Sarcasm in both cases helps me get through.
If you and I meet it will be the same. If you have a sense of humor, we might even laugh and for that moment everything will seem fine.